Pediatric Both Bone Forearm Fractures.

Pediatric both bone forearm fractures represent as much as 40% of pediatric fractures, with 60% occurring in the distal metaphysis, 20% in the midshaft, and 14% at the distal physis.
The most common mechanisms of injury are falls from height, sporting events, and playground injuries. 15% of fractures have a concomitant supracondylar fracture resulting in a "floating elbow"..

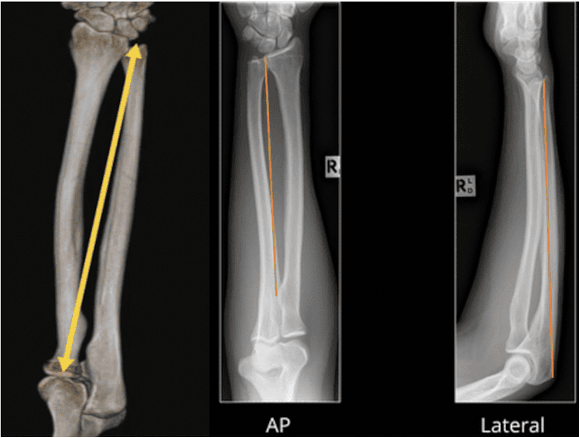
The rotational axis of the forearm runs between the radial head and ulnar fovea and a study by Hreha et al. found the mean coronal bow of the radius to be 14 ± 2.0 mm at 59% of the length and the mean sagittal ulnar bow to be 6 ± 3 mm at 39% of the length.
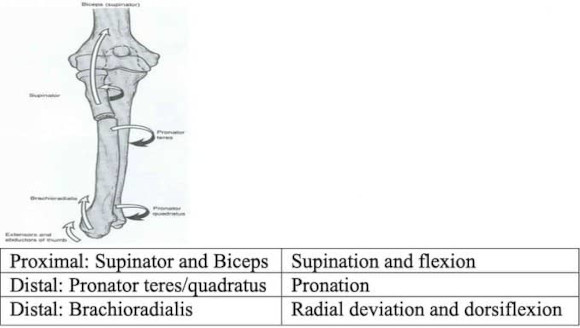
Deforming forces on radial fragments:
When assessing patients with bone forearm fractures it is important to perform a proper skin exam as they may present as subtle open fractures "poke hole". It is also important to assess for compartment syndrome via passive stretch as well as neurovascular status.

Malrotation can be assessed by checking cortical thickness and diameters of the fragments, and by checking for alignment of bony landmarks The radial styloid and bicipital tuberosity should be 180° apart on an AP The ulnar styloid and coronoid are 180° apart on a lateral view
Non-operative tolerances are based on age and can be remembered by the fact that the malrotation tolerances are 3x the angulation tolerances and bayonet apposition (shortening) is only tolerated in children < 10 y.o.

Casts should be oval shaped and wider in the coronal plane. The casting index may be utilized to reduce the risk of loss of reduction
The casting index is the diameter of the cast in the sagittal plane / diameter in the coronal plane and it should ideally be less than 0.8. It is more challenging to obtain a CI < 0.8 in proximal fractures due to increased soft tissue.
Flexible IM nails: radial nail should be placed first through the radial styloid. The ulnar nail may be inserted either retrograde (through the ulnar styloid) or anterograde (through the olecranon).
ORIF with plate/screws: typically used in adult BBFFs may be required in some instances. An interval to the ulna may be made between the FCU & ECU and the Volar Henry approach may be used to access the radius.
When using a single incision, patients are at an increased risk of synostosis, ossification of the interosseous membrane, occurring in 3-9%. Excision should be performed after the tissue have matured, after 4-6 months, though excision rarely improves function
Functional results depend on restoration of the radial bow. Malunion resulting in angulation > 20 degrees is likely to impair forearm rotation. Multiple attempts to pass flexible nails may increase the risk of compartment.
References:
1: https://journals.lww.com/clinorthop/fulltext/2020/01000/what...
2: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4510792/
3: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3453027/pdf/...
4: https://www.wheelessonline.com/trauma-fractures/closed-redu...
Full Review and Conversation on X