If you're interested in orthopedics you won't want to miss this one!

Clavicle fractures are typically the result of a fall onto the shoulder and are one of the most common fractures in children.
They may also occur from direct trauma, seizures, or a fall onto an outstretched hand (FOOSH).
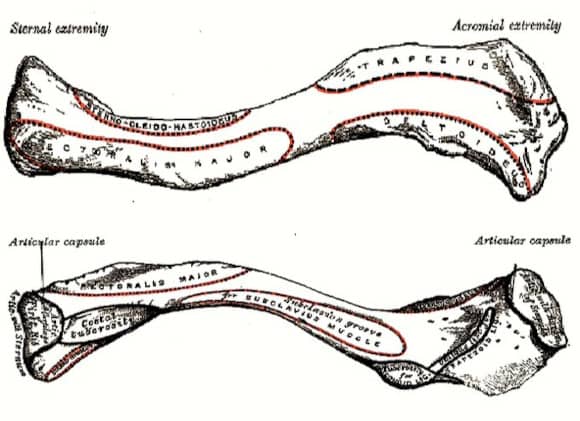
The clavicle serves as the connection between the UE and axial skeleton.
It is the first bone to ossify and the last to fuse. It is S-shaped and widest medially.
Most fractures occur in the middle 1/3rd, roughly 80%, which is the thinnest segment.
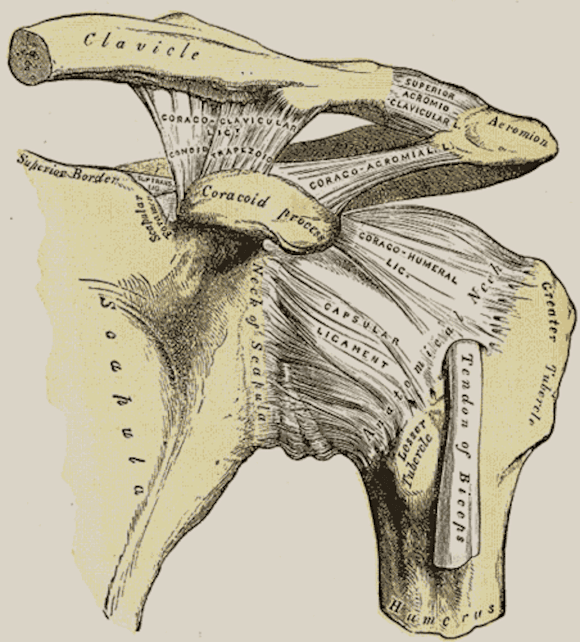
Which of the coracoclavicular ligaments is more medial?
Conoid / trapezoid
The conoid ligament is approximately 4.5 cm medial to the AC joint whereas the trapezoid is approximately 3 cm.
This can be remembered as they go in alphabetical order from medial to lateral.
The CC ligaments play an important role in the stability of distal clavicle fractures.
Physical exam:
✯ Assess for skin tenting (pending open fx)
✯ Lung Auscultation (r/o pneumothorax)
✯ Careful neurovascular exam
-Although rare it must be ruled out with many important neurovascular structures posterior/inferior to the clavicle

Imaging:
Most clavicle fractures can be confirmed by AP chest radiograph.
In addition, a clavicle series should be obtained consisting of an AP clavicle and AP cephalic tilt view (15-30° cephalad tilt) which reduces thoracic overlap.

The Allman-Neer Classification is commonly used for clavicle fractures.
Dr. Allman initially classified clavicle fractures as:
Group 1: Middle 1/3 (80%)
Group 2: Distal 1/3 (15%)
Group 3: Proximal 1/3 (5%)
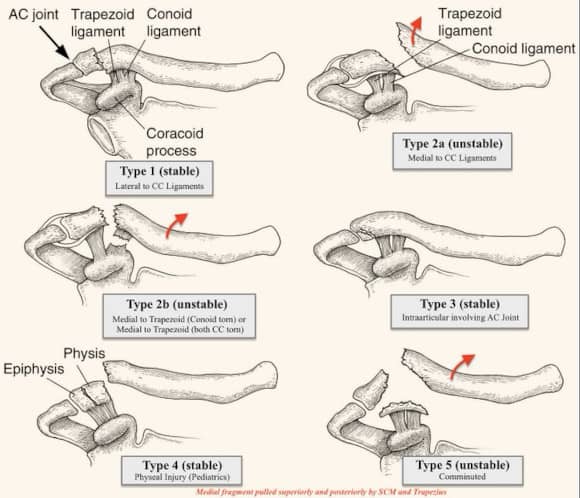
Dr. Neer further categorized distal 1/3 fractures (group 2) into 5 types
Group 2 (Distal 1/3):
Type 1: Lateral to CC ligaments
Type 2a: Medial to CC ligaments (CC intact)
Type 2b:
-Medial to trapezoid (conoid torn)
-Medial to trapezoid (both CC torn)
Type 3: Intraarticular involving AC joint
Type 4: Physeal injury (pediatric)
Type 5: Comminuted
Non-operative Management:
The majority of minimally displaced clavicle fractures may be treated with either a sling or figure 8-brace.
Slings work by raising the lateral fragment superiorly and posteriorly.
Figure-8 braces work by depressing the medial fragment.

Studies have shown that slings and figure-8 braces produce similar results while slings are more comfortable and produce fewer skin problems.
Though figure-8 braces allow the use of both arms and may be beneficial in children that may frequently take their slings off.
Operative indications:
✯ Neurovascular injury
✯ Skin tenting
✯ Open fracture
Controversial Indications:
✯ Unstable distal 1/3 fractures
✯ Z-deformity (Kickstand fragment)
✯ Comminuted fractures
✯ > 2 cm shortening
✯ > 100% displacement

Operative Management:
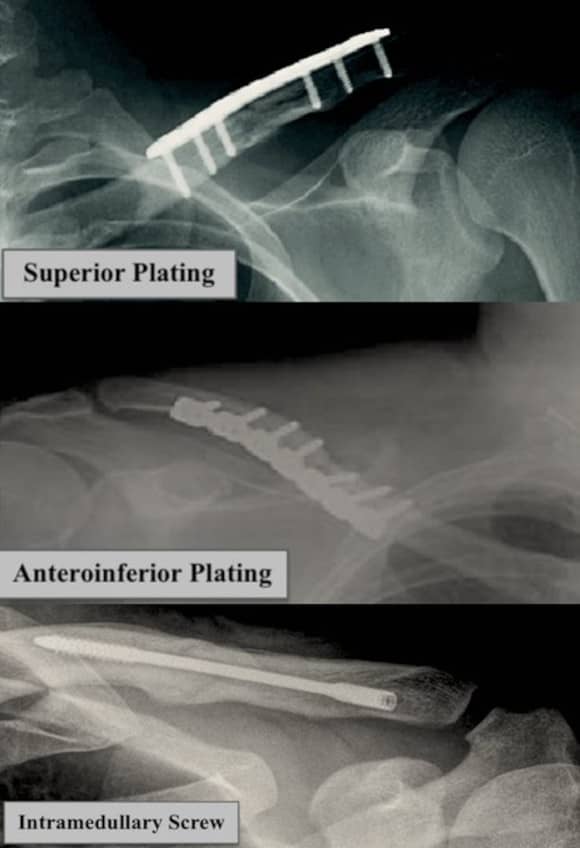
✯ ORIF with plate and screws
✯ CR with intramedullary fixation
Plates may be placed either superiorly or anteroinferior.
Which plating position is biomechanically stronger?
Superior/anteriorinferior
Superior plating is biomechanically stronger, while anteroinferior plating may be associated with lower rates of hardware prominence.
Operative vs non-operative management:
✯ Faster time to union
✯ ↓ rate of cosmetic deformity
✯ 1 in 4 patients request hardware removal
Complications:
✯ Hardware Prominence
✯ Cosmetic deformity
✯ Non-union
✯ Malunion
✯ Infection